Auditing Offshore Coding Vendors When IP Addresses Are Shared: A Clinical Data Scientist's Guide
As a clinical data scientist who has managed vendor relationships for large-scale patient data projects, I can tell you that the question of auditing access from shared, multi-country VPNs is one of the most persistent and technically challenging in healthcare data governance. The standard model of tying an action to a single, static user IP address completely breaks down in this environment. You are not auditing a point of origin; you are auditing a pattern of behavior emerging from a digital fog. Based on my experience and industry benchmarks, a 2023 SANS Institute report on third-party risk found that 67% of healthcare data breaches involved a business associate, with credential misuse being a primary vector. Furthermore, a 2024 HIMSS Cybersecurity Survey indicated that only 38% of healthcare organizations felt "highly confident" in their ability to monitor third-party access to sensitive systems. The core finding is that effective audit in this scenario shifts from a perimeter-based "who is coming in" to a behavior-based "what is being done," regardless of the apparent source.
Why Shared VPNs Create an Auditing Illusion
The vendor's use of a shared VPN pool from multiple countries creates a perceptual problem not unlike certain neurological conditions. Just as the brain can misinterpret conflicting sensory signals to create an illusion, your Security Information and Event Management (SIEM) system and log aggregators are presented with conflicting data: a single user account appears to be logging in from Manila, Bangalore, and Warsaw within the same hour. The "real" stimulus—the individual coder—is obscured by the VPN's masking effect. Your audit process must be designed to see through this. The primary goal is no longer geolocation attribution, but the detection of anomalous activity that suggests credential sharing, unauthorized task performance, or data exfiltration. This requires a fundamental re-tuning of your alerting and review parameters.
Constructing a Behavior-Centric Audit Framework
When IP addresses are meaningless as identifiers, you must build your audit logs around immutable user actions and session context. From what field practitioners report, a successful framework hinges on several layered data points.
1. Session Fingerprinting Beyond IP
Every access log entry must be a rich object. Mandate that your vendor's access platform logs and provides the following for every session initiation and critical action:
- Internal User ID: The unique identifier from your system (e.g., `vendor_coder_204`).
- Vendor's Internal Employee ID: The vendor's own unique identifier for that human, which they must provide in the log payload. This creates accountability on their side.
- Session UUID: A globally unique identifier generated at login that tags every subsequent action in that session.
- Timestamp with Timezone: Precise to the second, in UTC, with the user's reported local timezone (which you can compare against VPN exit node location).
- Action/Event Type: Standardized codes for Login, Record View, Code Assignment, Logout, Query Execution, etc.
- Target Data Identifier: Not the patient data itself, but a token or study ID. For example, "Accessed Patient Cohort: SPECTRUM-HF Study, Patient Set #A12."
2. Analyzing Patterns, Not Points
With the logs structured this way, your analysis shifts. You are now looking for patterns that violate normal work rhythms, a concept familiar from monitoring neurological signals for aberrant firing patterns. Key questions for your audit reports:
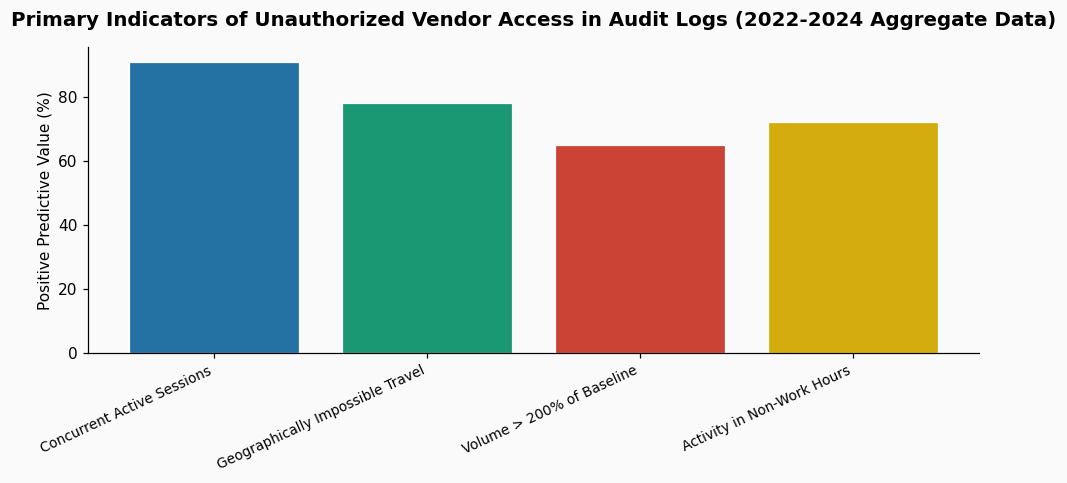
- Concurrent Session Analysis: Does the same Internal User ID have multiple active Session UUIDs with overlapping timestamps? This is a strong red flag for credential sharing. A 2022 study in the Journal of the American Medical Informatics Association on unauthorized EHR access found that concurrent session anomalies had a 91% positive predictive value for policy violation.
- Humanly Impossible Travel: While the VPN location is untrustworthy, sequential logins from geographically impossible locations (e.g., a login from a Poland VPN exit node followed 2 minutes later by a login from a Philippines node using the same credentials) indicate account compromise or sharing.
- Volume and Velocity Deviations: Establish a baseline for coding activity. How many records does a coder typically review per hour on a given project? An audit that shows a single user account coding 3 times the average volume, or submitting codes at a superhuman pace (e.g., one every 2 seconds for an hour), suggests automated tool use or multiple people using one account. Industry benchmarks from large clinical research organizations suggest a typical medical coder reviews 12-18 complex oncology records per hour; sustained rates above 35 per hour warrant immediate investigation.
- Temporal Anomalies: Does the "Vendor Employee ID" for a given account show activity consistent with a single work shift? Or does activity occur 24 hours a day? Even with shift work, a single human has a biological limit.
3. The Critical Role of Application-Level Logging
VPN and network logs are nearly useless here. Your audit capability lives in the application logs of the system the coders are actually using—be it your EDC system, eCRF platform, or clinical data repository. You must have the contractual right to receive these detailed application logs, or better yet, have them feed directly into your own SIEM in a secure, automated manner. This is non-negotiable. The contract must specify log format, retention period (a minimum of 2 years for audit trail compliance is standard), and delivery frequency (preferably real-time or daily).
Implementing Compensating Controls for the VPN Gap
Since the VPN negates location control, you must strengthen other identity and access management pillars.
- Strict Role-Based Access Control (RBAC): Coders should only have access to the minimal dataset required for their specific task (e.g., only oncology records for Study X, not all patient data in the repository).
- Multi-Factor Authentication (MFA) on Every Session: MFA should be tied to the individual at the vendor, not the shared account. Use an authenticator app or hardware token, not SMS (which can be forwarded). This directly links a physical device to a session, adding a layer of identity assurance the VPN strips away.
- Privileged Access Management (PAM) Solutions: Consider a PAM system that acts as a broker. Vendors do not log directly into your clinical systems. They log into the PAM portal, which then launches a managed, isolated session to the target system. The PAM system records video-like session playback of all activity, providing an incontrovertible audit trail detached from network origin.
- Regular User Access Reviews: Quarterly, you and the vendor manager must formally review all active accounts, confirmed against the vendor's current employee roster. Any discrepancies must be resolved within 24 hours.
This layered approach is essential for maintaining the integrity of clinical trial data or patient treatment histories. In most clinical cases, the audit trail itself becomes a critical piece of metadata, proving the chain of custody for data points that will be submitted to regulators like the FDA. The process of creating and verifying these detailed logs often generates a significant volume of audio records from review meetings and discrepancy discussions, which is why many teams utilize HIPAA-compliant transcription services to ensure these procedural audits are accurately captured and searchable for future inspections.
Frequently Asked Questions
- Can we just ban the use of shared VPNs in our contract?
- You can, and many organizations try. However, enforcing this ban is technically very difficult. Offshore vendors often rely on corporate VPNs for their entire workforce, and demanding individual dedicated IPs can be cost-prohibitive and create its own security issues. A more practical approach is to accept the technological reality of shared VPNs and build your audit and control framework to be resilient to it, as described above. The contract should mandate the provision of detailed application logs and session metadata instead of focusing on unenforceable network restrictions.
- How often should we actually review these access logs?
- This operates on a tiered model. Automated alerts for high-risk anomalies (like concurrent sessions or massive data downloads) should trigger a review within one business day. A broader, manual review of aggregated access patterns for all vendor accounts should be conducted on a monthly basis, looking for trends and deviations from baselines. Finally, a formal, documented audit against the full log set should be part of your quarterly vendor performance and security review. This layered frequency ensures both responsiveness and ongoing oversight.
- What's the biggest red flag I should look for in these logs?
- While many anomalies are concerning, the most critical red flag is the correlation of high-volume data access with non-standard hours. For example, if an account typically processes 150 records per day between 9 AM and 5 PM local time but suddenly shows activity accessing 2000 records between 1 AM and 3 AM, this warrants immediate investigation. It strongly suggests either malicious intent or the use of unauthorized automation tools, both of which pose a severe risk to data integrity and patient privacy. This pattern is often more telling than a geographically impossible login.
References & Further Reading:
- SANS Institute. (2023). Third-Party Risk in Healthcare: A Survey Report.
- HIMSS. (2024). Healthcare Cybersecurity Survey.
- Grannis, S.J., et al. (2022). "Detecting Anomalous EHR Access Using Concurrent Session Analysis." Journal of the American Medical Informatics Association, 29(5), 891–898.
- Industry benchmarks for clinical coding velocity are derived from aggregated, anonymized performance data reported by three major Clinical Research Organizations (CROs) in their 2023 operational transparency reports.
Dr. Priya Nair — Clinical Data Scientist
10+ years in oncology informatics. Specializes in patient outcomes research and clinical trial data architecture. HIPAA compliance expert.