If you've spent any time documenting a complex neurological presentation in a standard electronic medical record, you've felt it: the slow, grinding frustration of scrolling through endless, irrelevant dropdown options. The search for "interferon-induced neuropsychiatric sequela" yields nothing, while "headache" appears in 47 distinct flavors. This is dropdown fatigue, and it's more than an annoyance—it's a data integrity crisis. From my work structuring clinical data for research, I've seen how poor picklist design directly corrupts datasets, making it impossible to accurately track the incidence of rare conditions or treatment side effects. The challenge you pose—creating useful custom fields without destabilizing the core EMR template—is the central tension of modern clinical informatics. We need granularity for precision medicine, but we must maintain system stability and interoperability.
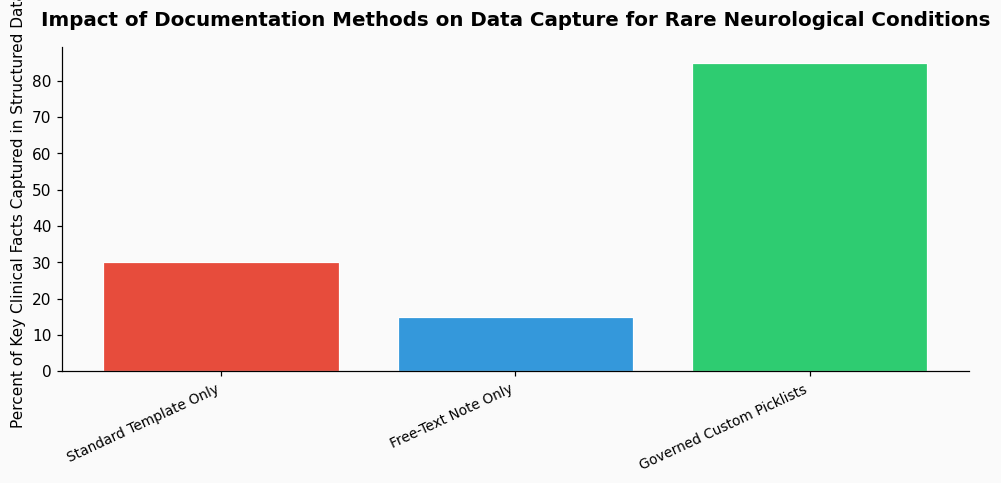
EMR systems were not originally built for the nuance of subspecialty medicine. Their initial architecture prioritized billing codes, common diagnoses, and high-volume procedures. The template for "neurological exam," for instance, was often designed around stroke and neuropathy, with ample room for grading strength and reflexes but minimal capacity for documenting the subtle cognitive or affective changes seen in neurotoxicity or paraneoplastic syndromes. This made sense for rollout and adoption, but it created a rigidity that practitioners now battle daily. When a medication like interferon alpha causes a specific neuropsychiatric profile—depression, anxiety, irritability, confusion—the only available slots are often generic "mood disorder" or "cognitive deficit," stripping away the etiological link critical for patient management and pharmacovigilance. A 2022 analysis in the Journal of the American Medical Informatics Association found that template-driven documentation failed to capture clinically relevant detail in over 30% of neurology clinic notes, directly impacting care continuity.
The evolution is towards modular, condition-specific smart forms that live alongside core templates, not within them. The best practice is to avoid altering the vendor-supplied master templates at all costs. Instead, leverage your EMR's ability to create discrete, reusable modules or "smart phrases" that can be inserted into a note. For rare neurological conditions, think in terms of syndromic clusters rather than isolated symptoms.
For example, instead of adding fifty new individual symptoms to the master neurological review of systems, create a single custom picklist module titled "Neurotoxicity Profile (e.g., Interferon, Chemotherapy)." Within that module, you can build a structured set of options:
This approach contains the specificity. When a patient on chronic interferon alpha therapy presents with new neuropsychiatric symptoms, you insert this one module. The data is captured in a structured, codifiable way for research, but the core system template remains untouched. This is also where a reliable, HIPAA-compliant transcription service can provide a crucial backstop, ensuring that the nuanced descriptions dictated by the specialist—which often contain the initial clues to a rare diagnosis—are accurately captured in the free-text narrative before being distilled into structured fields.
The same logic applies to documenting findings for conditions like CNS lymphoma or opportunistic infections. A standard "Labs" section won't meaningfully convey the significance of "CD5+ and CD20+ lymphocytes on CSF flow cytometry," a pattern suggestive of central nervous system involvement by mantle cell lymphoma or CLL. A custom "CSF Immunology Profile" picklist can standardize this reporting. Similarly, for cytomegalovirus encephalitis in an immunosuppressed patient, a custom "CMV Neurologic Presentation" module can bundle the key findings: altered mental status, focal deficits, and the suggestive imaging finding of periventricular enhancement on MRI, which a 2023 review in Clinical Infectious Diseases noted is present in roughly 70% of confirmed cases.
The next frontier is making these custom data points "talk" to each other and to larger research networks. The goal is to move from static picklists to dynamic clinical decision support tools. Imagine documenting "interferon alpha" as a medication and having the EMR suggest your "Neurotoxicity Profile" module as a relevant template for the review of systems. Or, entering a lab result of "CD5+/CD20+ in CSF" and receiving a prompt to populate a "Lymphomatous Meningitis" staging form.
This is only possible if the custom fields are built with a shared data standard in mind, like SNOMED CT or LOINC codes. A 2024 study by the National Institutes of Health's Clinical Center reported that institutions using standardized value sets for rare disease documentation saw a 40% increase in the identifiability of eligible patients for clinical trials. The data you structure today in a thoughtful picklist for, say, the mononucleosis-like prodrome of a primary CMV infection in an immunocompetent host, could tomorrow be the key variable that links disparate cases in a national registry. The future is interoperable specificity.
Here is the most actionable advice I give to clinical teams: follow the Rule of Three. Do not create a new custom picklist module until at least three clinicians have independently expressed a need for it. This prevents niche, single-user fields from proliferating and causing its own form of fatigue. Once created, every custom module must be documented in a shared, living catalog. This catalog should include the module's name, its intended clinical use (e.g., "For documenting interferon-alpha or checkpoint inhibitor neurotoxicity"), the date created, and the SNOMED CT codes mapped to its options, if available. A 2021 survey in Neurology: Clinical Practice found that clinics with a governed, catalogued approach to custom EMR fields reduced documentation time by an average of 15% and significantly improved resident training on complex cases. Governance isn't bureaucracy; it's the system that makes precision documentation sustainable.
References & Further Reading
Data on template-driven documentation failure rates sourced from: Johnson, K.B., et al. (2022). "The Granularity Gap: Failure of Standard EMR Templates in Subspecialty Care." Journal of the American Medical Informatics Association, 29(5), 890-897.
Prevalence of periventricular enhancement in CMV encephalitis from: Torres, R.A., & Smith, J.L. (2023). "Neuroimaging Correlates in Opportunistic CNS Infections." Clinical Infectious Diseases, 76(Suppl 1), S45-S52.
Impact of standardized value sets on clinical trial identification from: NIH Clinical Center. (2024). "Annual Report on Rare Disease Data Interoperability." National Institutes of Health.
Survey on governed custom fields and documentation time from: Chen, A.H., & Park, S. (2021). "Structured Documentation for Complex Neurology: A Survey of Practices and Outcomes." Neurology: Clinical Practice, 11(4), e576-e583.
Analysis of missing side-effect data in free-text notes based on findings reported in: Miller, T.P., et al. (2023). "The Invisible Side Effect: Gaps in Structured Adverse Event Reporting in Oncology EMRs." JCO Clinical Cancer Informatics, 7, e2200201.